Get in touch 020 7042 1888 | imaging@oryon.co.uk



Swimming: what are the risks?
With Dr Mike Burdon, Consultant in Sport, Exercise and Musculoskeletal Medicine

Swimming: what are the risks?
Posted on Thu Sep 5, 2019
Swimming is a fantastic sport and exercise, both at elite and at recreational level. It provides an excellent holistic exercise, combining aerobic training in a non-impact environment with resistance training through the water. At recreational level it provides great exercise for all; especially for people who perhaps need a lower impact option than running or fast walking. The variety of techniques available mean that people can almost always gain fitness benefits from swimming.
However, as with any exercise, medical problems can occur. The incidence of such problems increases as the volume of training increases, but for the benefit of this article we will discuss them in general, as they may be applicable to all swimmers, whatever the level.
Medical conditions in swimming
Medical issues may be seen in any sport or exercise, but there are some which appear to be more common in swimming.
Asthma and swimming
Asthma is a common condition that affects many people in general, with a higher incidence in swimmers. Various studies have reported that it may be seen in 40-75% of swimmers, with highest rates seen in elite swimmers. A particular form of asthma is known as exercise-induced asthma or bronchoconstriction. Here, typical symptoms of asthma such as coughing, wheezing and shortness of breath are classically seen after exercise has started. This can lead to significant issues for susceptible swimmers, affecting performance and quality of life. There are several reasons why this may occur.
Firstly, the asthma may be linked to allergy. Rhinitis and nasal allergy are common- they may be linked to the presence of chloramines in the water. Chloramines form when the chlorine reacts with nitrogen- containing compounds in the water- these may be due to swimmers not showering before entering the pool with consequent urine/sweat being present. The chloramines may lead to various symptoms affecting the eyes, skin and respiratory symptoms.

Public hygiene such as showering and well-ventilated pools are very important to reduce the incidence of issues. Allergy symptoms can be controlled with antihistamines and nasal sprays where needed. Asthma symptoms are likely to need an inhaled bronchodilator for symptom relief and prevention, with steroid inhalers plus other medications such as Montelukast often being required.
Secondly, exercise-induced asthma is also related to the volume of training and time spent in the pool environment, hence the higher incidence seen in elite swimmers who train for many hours per week.
Swimming-related injuries
Swimming injuries can affect various regions of the body, but as may be expected are seen with higher incidence to affect the shoulder. Other regions that may be affected include the elbow, back, neck and knee. For this article we will consider shoulder and knee injuries.

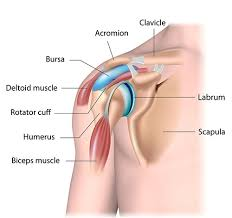
Shoulder injuries
The shoulder is of course hugely important in an activity such as swimming. It has been estimated to affect nearly 80% of elite swimmers at some point in their career. There are various joints that comprise overall shoulder joint complex; the glenohumeral joint being the most important. This is a ball-and-socket joint that provides a wide range of joint mobility, thus enabling the shoulder to have a huge range of movement. This is of course vital in swimming. The biomechanics involved in each shoulder will vary with each stroke/technique and should be considered in any case of injury (outside the scope of this article).
The rotator cuff represents a collection of tendons that attach muscles to the humeral head and are vital in controlling glenohumeral joint movement. With regular use and overuse the tendons can become subject to high loading tensile forces. Tendon overuse and muscle fatigue may combine to alter kinematics of the shoulder and lead to subacromial impingement. This may be further increased by a high degree of shoulder laxity that can be seen in many swimmers; this shoulder instability being an important part of the aetiology (cause) of cuff issues. As well as assessing shoulder range of movement and performing specific cuff tests, examination for shoulder stability is also of high importance.
Investigations such as diagnostic ultrasound, X-rays and MRI may be needed in some cases to help diagnosis. Treatment will almost always include physiotherapy to address any muscle or cuff weakness, as well as providing rehabilitation for instability as needed. Close liaison with swimming coaches to correct any contributing biomechanics with swimming technique is often required. In younger swimmers where growth plates are still open, a rest from swimming or at least a significant reduction in training volume may be essential. For some swimmers across age groups, medications, steroid/hyaluronic acid injections and shockwave therapy may be adjuncts to recovery to also consider.
Older swimmers may develop other issues such as osteoarthritis of the GHJ/ACJ, frozen shoulder (capsulitis), cervical radiculopathy leading to referred pain and degenerative labral pathology.
The glenohumeral joint (GHJ) and acromioclavicular joint (ACJ) may also develop specific injury in swimmers. In older swimmers osteoarthritis of the ACJ especially may occur. This will usually present with very localised pain on the top of the shoulder. Physiotherapy is usually required and sometimes a steroid injection may also help relieve pain. Less commonly, surgery may be performed if the pain is causing restricted activity on an ongoing basis.
Knee injuries
The knee may also be injured during swimming, although the incidence is much lower than with other impact exercise. It is difficult to know the true incidence of knee injury, due to limited data and studies, but is thought to occur in 10-20% of elite swimmers as an estimate. The most common sites of knee pain are medial (seen in breaststroke) and anterior knee representing patellofemoral pain.
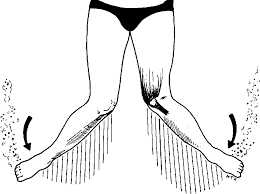
Of course, each swimming stoke has its own unique biomechanical factors present; in breaststroke the knee rapidly extends from a flexed position with additional external rotation of the lower leg. This generates a high valgus load as a result and may lead to strain/overuse of the medial knee structures. This is often referred to as “breaststroker’s knee.” This largely represents strain of the medial collateral ligament (MCL) but may also represent pes anserine bursopathy, meniscal injury, medial compartment chondropathy and other medial knee bone stress.
Investigations may be needed and may include X-ray to assess bone and joint space, with MRI providing a more comprehensive assessment including ligament, bone, cartilage and other structural detail. Treatment may include relative rest, modification of technique with interventions such as injections and surgery in rarer cases.
It is important to know about breaststroker’s knee if you already have knee pain and are starting to swim. I will often prescribe swimming as an exercise for patients with arthritis and other knee conditions, but I advise that breaststroke may aggravate pain when medial knee issues are present. Swimming with a float between the knees may negate this issue, as may using other strokes such as freestyle/backstroke, noting that that these are generally more of a technical challenge for some new swimmers.
Patellofemoral pain is less commonly seen in swimming than in dry land sports but may still occur, especially when elite swimmers train in the gym or run for other exercise. Pain may also be felt pushing off during swimming laps. The condition is usually managed with physiotherapy/rehabilitation with correction of any contributing biomechanical factors.
Would I recommend swimming?
Yes, absolutely. Swimming is a fantastic exercise that may benefit people of all ages. As with any exercise or sport injuries do occur but in general occur less frequently than with other sports. The health benefits of swimming far outweigh the potential risks of injury, which are more commonly seen in elite swimmers where the volume of training is significantly higher.
Dr Michael S. Burdon is a Consultant in Sport, Exercise and Musculoskeletal Medicine. He practices at Pure Sports Medicine in London.
Have you suffered an injury, or do you live with pain? Contact Oryon Connect to be introduced to an expert healthcare professional, who can see you for an affordable consultation quickly and efficiently.
At Oryon Connect, we can help guide you through your healthcare journey, offering affordable appointments with practitioners, as well as affordable and efficient diagnostic imaging if needed.
Share this article
Most Recent
What To Expect From a Prostate MRI
Posted on Fri Oct 3, 2025
Interview with Our Referral Relationships Manager
Posted on Fri Oct 3, 2025
Posted on Tue Sep 16, 2025
